Brow Thread Lift Case Study: Lateral Brow Descent


A patient in her late 40s presented with lateral brow descent that gave her a tired, heavy upper-eye look despite a calm rest face. This case study walks through the PDO thread placement plan that lifted the outer brow back into a youthful angle without an upper-lid blepharoplasty.
Case Overview
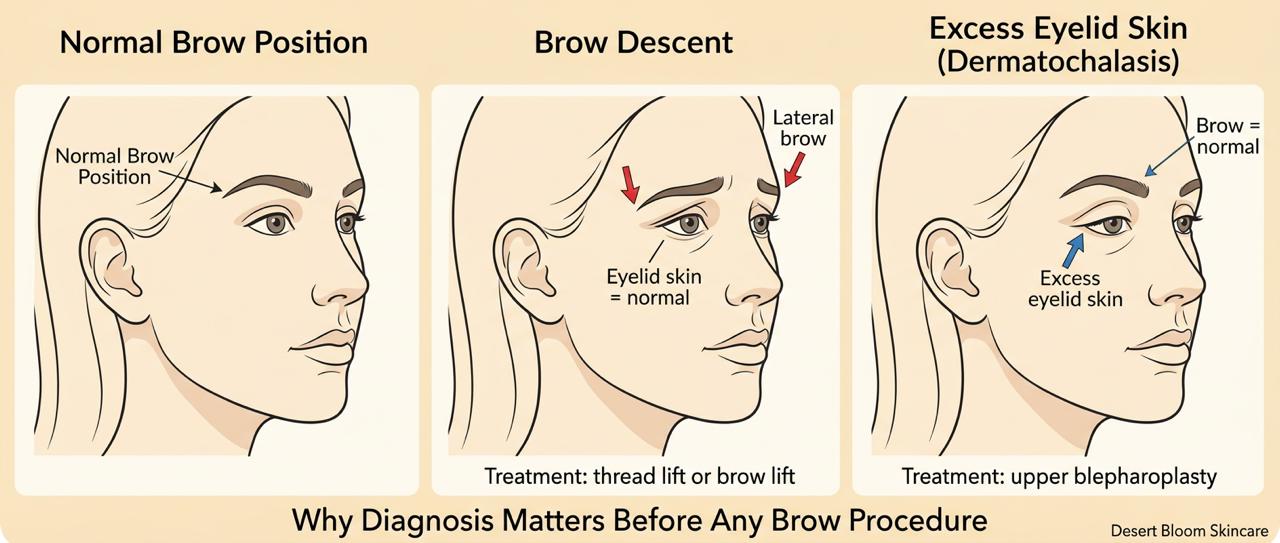
Most patients who come in describing heavy upper eyelids have never been told there are two very different conditions that look nearly identical in the mirror. This case follows a 65-year-old woman whose upper eyelid heaviness was primarily driven by lateral brow descent — a distinction that changed both the diagnosis and the treatment plan entirely. Threading the wrong anatomy does not fix the problem. Accurate diagnosis before any procedure is selected is the difference between a meaningful result and a wasted intervention.
This brow thread case is part of our case studies library at Desert Bloom, alongside the 6-month facial fatigue thread lift case and our jawline contouring case study. For treatment information, see our full PDO thread lift and non-surgical brow lift pages.
Case Snapshot
- Patient
- 65-year-old woman
- Concern
- Heavy upper eyelids, lateral brow descent
- Treatment
- PLLA/PCL absorbable thread lift with neuromodulator preparation
- Anesthesia
- Local, in-office
- Key Finding
- Brow descent — not eyelid skin excess — was the primary driver, which changed the treatment plan entirely.
- Longevity
- 12 months to several years in appropriately selected patients
Patient Background and Clinical Presentation
This case involves a 65-year-old woman who presented with concerns about heavy upper eyelids and a drooping brow, particularly laterally. Her primary complaint was visual and aesthetic fatigue rather than eyelid skin redundancy alone.
A comprehensive assessment was essential to determine whether her symptoms were driven by brow descent, upper eyelid skin excess, or a combination of both. This distinction matters: the two conditions can look nearly identical to the patient, yet require entirely different interventions. Threading the wrong anatomy does not fix the problem — it wastes the patient’s time and money and may delay appropriate care.
Treatment Planning
Treatment Planning and Clinical Rationale

Multiple treatment options were reviewed at consultation, including neuromodulators alone, surgical brow lift, upper blepharoplasty, and non-surgical brow repositioning with absorbable threads. After evaluation, we determined that brow descent was a significant contributor to her symptoms. A decision was made to proceed with non-surgical brow repositioning using absorbable sutures, with a clear and shared understanding of goals and limitations between provider and patient.
Not every patient requesting brow threads is an appropriate candidate. Some patients who perceive brow heaviness actually have a normally positioned brow and a primary concern related to excess upper eyelid skin. In those cases, upper blepharoplasty — not threads — is the appropriate treatment. Thread lifting cannot remove excess eyelid skin and should never be used as a substitute for surgical correction when skin redundancy is the primary issue. The four options reviewed at consultation:
- Neuromodulators alone — can create passive brow elevation but insufficient when true brow descent is present
- Surgical brow lift — definitive and durable, but overtreatment when anatomy doesn’t require it
- Upper blepharoplasty — appropriate when excess eyelid skin, not brow descent, is the primary problem
- Non-surgical brow repositioning with absorbable threads — selected here; mechanical repositioning appropriate to her anatomy
Why Neuromodulator Preparation Matters
In Dr. Borakowski’s protocol, neuromodulator treatment is administered to the forehead and brow depressor muscles before thread placement. This is a foundational component of the plan — not an optional add-on.
- Active forehead and brow muscles can work against thread vectors, particularly during the early healing phase.
- Muscle relaxation reduces mechanical stress on the threads while tissue settles.
- Relaxed musculature may help reduce the risk of early thread migration or premature softening of the lift.
In Dr. Borakowski’s clinical protocol, thread placement without prior neuromodulation may increase the risk of suboptimal or shorter-lived results. In this patient, pre-treatment with a neuromodulator was scheduled before the thread appointment as a foundational component of the plan, not as an optional add-on.
Procedure Details
Procedure Details: Thread Selection and Technique
PLLA/PCL absorbable threads were placed in-office under local anesthetic to support lateral brow repositioning. Thread selection was driven by patient age and tissue laxity — not a default protocol. PLLA/PCL was chosen specifically for this patient because of its greater tensile strength compared to PDO alone, longer-lasting structural support suited to age-related tissue laxity, and collagen stimulation along the thread pathway.
For younger patients with milder laxity, PDO threads may be entirely appropriate — thread selection should follow anatomy, not a default product. In this case, the degree of tissue laxity at age 65 made PLLA/PCL the clinically appropriate choice. For a fuller explanation of candidacy, technique, recovery, and pricing, see our brow lift treatment page.
For younger patients with milder laxity, PDO threads may be entirely appropriate — thread selection should follow anatomy, not a default product. In this case, the degree of tissue laxity at age 65 made PLLA/PCL the clinically appropriate choice. For a fuller explanation of candidacy, technique, recovery, and pricing, see our brow lift treatment page.
Recovery, Expected Side Effects, and What to Watch For
The forehead and brow region are highly vascular, making bruising a common and expected part of recovery — not a complication. Patients are counseled directly on this distinction so they are not alarmed by what is a normal healing response.
Common early side effects include:
- Bruising — common and expected; the region’s vascularity makes it difficult to avoid entirely
- Swelling and tenderness along thread paths, peaking around day 2
- Temporary tightness when raising the brows
- Small entry-point marks that heal quickly
- Initial rippling or slight puckering near the outer brow as tissue settles (typically resolves within 1–2 weeks)
Many patients can resume desk work within 24–48 hours. To minimize excessive bruising and prolonged recovery, patients are advised to:
- Discontinue blood-thinning medications or supplements — such as aspirin, ibuprofen, and fish oil — at least one week prior, only if approved by your prescribing provider; do not stop prescribed medication without medical guidance
- Avoid alcohol before the procedure, as it increases both bleeding and inflammation
- Avoid heavy exercise, saunas, and swimming for 1–2 weeks post-procedure
- Avoid pressing, rubbing, or sleeping face-down on the treated area for 2–3 weeks
- Avoid aggressive energy-based treatments over the brow for at least 6–8 weeks
Day 0–1
Procedure & Immediate Recovery
Threads placed under local anesthetic in-office. Expect bruising and swelling in the brow and forehead region. Ice packs and head elevation recommended. Resume desk work as tolerated.
Days 2–7
Peak Swelling Resolves
Swelling and tenderness along thread paths typically peak around day 2 then subside. Minor rippling or puckering near the outer brow is normal as tissue settles.
Day 14
Initial Results Visible
Entry-point marks largely healed. Brow position becomes more apparent. Most patients presentable for social settings.
Month 1–3
Tissue Integration
Threads integrating with surrounding tissue. Collagen stimulation along thread pathway begins. Neuromodulator effects still active, supporting the mechanical lift.
Month 12+
Long-Term Maintenance
Results in appropriately selected patients may last 12 months to several years. Maintenance typically considered every 24 months, tailored individually. PLLA/PCL threads fully dissolved, collagen scaffold persists.
When to Call Your Provider: Red Flag Symptoms
Most recovery from brow thread procedures is uneventful. However, contact the clinic promptly — same day — if you experience any of the following:
- Severe or worsening pain beyond the expected mild tenderness, especially if it intensifies after day 2
- Dusky or bluish discoloration in or around the brow or upper eyelid (possible sign of vascular injury)
- Signs of infection: increasing redness, warmth, swelling after day 3, discharge from entry points, or fever
- Visible thread exposure through the skin
As with all thread-based procedures, infection — while uncommon — is the most serious potential complication. Strict adherence to aftercare instructions and prompt communication with your provider are the most reliable protections.
Results
Longevity of Results

Results from non-surgical brow repositioning can vary widely and are influenced by patient age, degree of skin and tissue laxity, skin quality, and overall health and healing capacity. In appropriately selected patients, results may last anywhere from 12 months up to several years — though outcomes are not permanent and should not be compared to surgical brow lift results.
Absorbable threads dissolve over time, but the collagen scaffold they stimulate can help maintain some support beyond the thread’s lifespan. Patients with very expressive foreheads, significant sun damage, or strong brow depressor muscles may notice the lift soften sooner. Maintenance is typically considered every 24 months, tailored individually rather than on a rigid schedule.
In some patients, thread retreatment may be combined with other supportive treatments when volume loss, skin quality, or surrounding facial structure contributes to the concern. Those decisions are made individually after examination, not by default protocol.
How Non-Surgical Brow Repositioning Compares to Other Options
Many patients arrive asking whether threads, neuromodulators, or fillers are “better” for the brow area. The answer depends entirely on what’s driving the problem — they address different aspects of facial aging.
| Approach | Best When | Cannot Address | Used in This Case? |
|---|---|---|---|
| Neuromodulators alone | Early brow heaviness, dynamic descent | True structural brow descent | Yes — as pre-treatment prep |
| Absorbable thread lift | Static lateral brow descent, adequate elasticity | Excess eyelid skin | Yes — primary treatment |
| Temple filler | Volume loss contributing to descent | Structural brow repositioning | No — not indicated here |
| Upper blepharoplasty | Excess upper eyelid skin is primary concern | Non-surgical option cannot substitute | No — not the primary driver |
| Surgical brow lift | Significant descent, skin redundancy | Avoided here — overtreatment | No — anatomy didn’t require it |
Best When
- Neuromodulators alone
- Early brow heaviness, dynamic descent
- Absorbable thread lift
- Static lateral brow descent, adequate elasticity
- Temple filler
- Volume loss contributing to descent
- Upper blepharoplasty
- Excess upper eyelid skin is primary concern
- Surgical brow lift
- Significant descent, skin redundancy
Cannot Address
- Neuromodulators alone
- True structural brow descent
- Absorbable thread lift
- Excess eyelid skin
- Temple filler
- Structural brow repositioning
- Upper blepharoplasty
- Non-surgical option cannot substitute
- Surgical brow lift
- Avoided here — overtreatment
Used in This Case?
- Neuromodulators alone
- Yes — as pre-treatment prep
- Absorbable thread lift
- Yes — primary treatment
- Temple filler
- No — not indicated here
- Upper blepharoplasty
- No — not the primary driver
- Surgical brow lift
- No — anatomy didn’t require it
Clinical Perspective
This case highlights the importance of accurate diagnosis and restraint in aesthetic medicine. The temptation to proceed with a requested procedure must always be weighed against whether that procedure actually addresses the patient’s anatomy.
Non-surgical brow repositioning can be an effective option for selected patients with true brow descent, but it requires:
- Proper muscle preparation with neuromodulators before thread placement
- Appropriate thread selection based on patient age, tissue quality, and longevity goals
- Honest communication about what threads can and cannot achieve
- Acceptance of anatomical and procedural limitations — including referral to surgery when indicated
When these factors are respected, results can be supportive and meaningful without overpromising outcomes that only surgery can deliver. The goal of aesthetic medicine is not to perform every procedure a patient requests — it is to deliver the right procedure for the right patient at the right time.
“The most important step in a brow thread case isn't the technique — it's the diagnosis. A patient with excess eyelid skin will not benefit from brow threads, and doing the wrong procedure doesn't just fail to help — it delays the care that would actually work.”
Is Non-Surgical Brow Repositioning Right for You?
This case study represents one carefully selected patient — not a universal template. Candidacy depends on your specific brow anatomy, skin quality, and whether your concern is truly driven by brow descent or by another structural factor like excess eyelid skin.
At Desert Bloom Skincare Center in Scottsdale, AZ, Dr. Natalya Borakowski, NMD personally evaluates every patient before recommending a brow lift approach. All thread lift procedures are personally planned and performed by Dr. Borakowski. View our full case studies library to explore additional clinical scenarios.
Frequently Asked Questions
Can absorbable threads lift the brow if I also have excess eyelid skin?
Why is neuromodulator preparation required before thread placement?
Why were PLLA/PCL threads chosen instead of PDO for this patient?
How long can results realistically last at this patient's age?
What are the most important warning signs to report after a brow thread procedure?
Other Case Studies



