Fat transfer to face gone wrong

The artical is about discussing the topic of facial injection complications, their causes and how to prevent them. The article emphasizes that injectable procedures always carry risks and that anyone who claims the procedure to be risk-free should be avoided. The most common complications of injectable procedures, including facial fat transfer, are bruising and skin infection. The article gives recommendations on how to prevent these complications, such as stopping the use of blood-thinning agents before the procedure, using cannulas during facial injection, and following proper skin hygiene during and after the procedure.
When Fat Transfer Doesn’t Go as Planned
You did the research. You chose a qualified surgeon. You went through the recovery — the bruising, the swelling, the weeks of waiting to see results. And yet something is off. Maybe one side looks different from the other. Maybe there are lumps you can feel under the skin. Maybe the volume you gained in the first weeks has mostly disappeared. If any of this sounds familiar, you are not alone — and you deserve a clear explanation of what happened, what it means, and what options exist.
At Desert Bloom, we do not perform fat transfer. It is a surgical procedure requiring an operating room, anesthesia, and the infrastructure of a plastic surgery practice — none of which we have, and none of which we would try to replicate with injectables alone. What we do offer is an honest conversation about where fat transfer complications come from, what recovery really looks like, and when — and how — injectable options can help patients who are navigating an imperfect result. This guide is written for you: whether you are considering fat transfer and want to go in with open eyes, or you have already had it and something has not gone as expected.
What Goes Wrong & When to Act
- Common Issues
- Overcorrection, asymmetry, lumps, fat necrosis, resorption, migration
- When to Act
- Persistent lumps after 3 months, visible asymmetry, skin changes, or hardened nodules — seek evaluation
- Reversal Options
- Depends on complication — surgical revision, steroid injection, or complementary injectables to rebalance
- Why We Don't Offer It
- Fat transfer requires surgical infrastructure; Desert Bloom refers to board-certified plastic surgeons
- Related Reads
- Botched Treatment Guide · Thread Lift Gone Wrong · Dermal Fillers at DB
Why Fat Transfer Complications Happen

Fat transfer to the face — also called autologous fat grafting or lipofilling — involves harvesting fat from one part of the body, processing it, and injecting it into facial areas like the cheeks, temples, under-eyes, or jawline. It offers a permanent, biocompatible volume replacement — in theory. The biology is simply less cooperative than most surgical consultations acknowledge. The grafted fat must establish a new blood supply within the recipient tissue. When that process is incomplete — which happens more often than patients are told — fat cells die, and the complications begin.
Technique matters enormously: the harvesting method, the centrifugation process, the injection depth and volume, the surgeon’s anatomical precision. Candidacy matters just as much. Patients with thin skin, poor tissue vascularity, or a history of significant weight fluctuation are at higher risk for uneven resorption. Post-procedure factors — sun exposure, infection, physical trauma to the treated area — can derail results that looked perfect at the three-week mark. When something goes wrong, it is rarely one single cause. It is usually a combination of variables that were difficult to predict and harder to control.
The Most Common Complications — What They Look Like and What Causes Them
Not all fat transfer complications are created equal. Some resolve on their own. Others require intervention. Here is what patients most commonly experience:
Overcorrection
→Discuss correction — The surgeon placed more volume than the tissue could accommodate, or the initial swelling masked the true final result. This typically becomes visible at 4–8 weeks.
Asymmetry
→Discuss correction — One of the most common outcomes — fat resorbs at different rates on each side of the face, or uneven injection volumes create a visible imbalance.
Lumps and nodules
→Discuss correction — Clusters of fat cells that did not integrate evenly. These can feel firm or soft, be visible in certain light, and may persist for months.
Fat necrosis
→Discuss correction — Dead fat tissue forms a firm, sometimes painful mass. In mild cases, it resolves over months. In more significant cases, surgical excision may be needed.
Oil cysts
→Discuss correction — When fat cells rupture, the released lipids can form a fluid-filled pocket beneath the skin. These are usually benign but often require drainage.
Under-correction (resorption)
→Discuss correction — A significant portion of the grafted fat is naturally resorbed by the body. Some surgeons anticipate this and intentionally overcorrect; others do not. The result can be a final volume that falls far short of what was planned.
Migration
→Discuss correction — Fat that shifts from the intended injection site to adjacent tissue, creating volume in unexpected places — most commonly in the lower cheeks or along the jawline.
Recovery After Fat Transfer — The Real Timeline

The gap between what patients are told before a fat transfer and what they experience during recovery is, honestly, one of the most consistent patterns I hear about in consultations. Swelling in the first two to four weeks can be dramatic — and it is supposed to be. The body is responding to both the harvest site trauma and the injection sites simultaneously. During this period, it is nearly impossible to assess the final result, and any attempt to do so creates anxiety that is mostly unwarranted. The appropriate response in those early weeks is patience, not intervention.
The challenging phase begins at months two through four, when the initial swelling resolves and the true volume becomes visible — along with any asymmetries, irregularities, or resorption. This is the window when most patients contact their surgeon with concerns. If the outcome is within the expected variation range, additional fat grafting sessions are typically recommended (fat transfer is commonly performed in multiple rounds precisely because of resorption). If the outcome involves a complication — necrosis, a persistent cyst, significant asymmetry — the path forward depends on the nature and severity of the issue.
Days 1–5
Peak Swelling
Both harvest and injection sites are swollen and bruised. Sleeping elevated, avoiding pressure. No assessment of results is meaningful at this stage.
Weeks 2–4
Swelling Resolving
Bruising fades. Swelling begins to decrease. Some initial 'lumpy' texture is normal as fat integrates. The result is still not final.
Months 1–3
Resorption Phase
The body naturally resorbs a portion of grafted fat — typically 30–50%. Asymmetries and under-correction become visible. This is when most complications are identified.
Months 3–6
Stabilization
Volume stabilizes. Fat that has survived to this point is largely permanent. Persistent lumps, nodules, or asymmetries at this stage warrant evaluation.
6 Months+
Final Result Assessment
True final result. If complications remain — significant asymmetry, necrosis, oil cysts — a corrective plan can now be accurately developed.
What Desert Bloom Can Offer
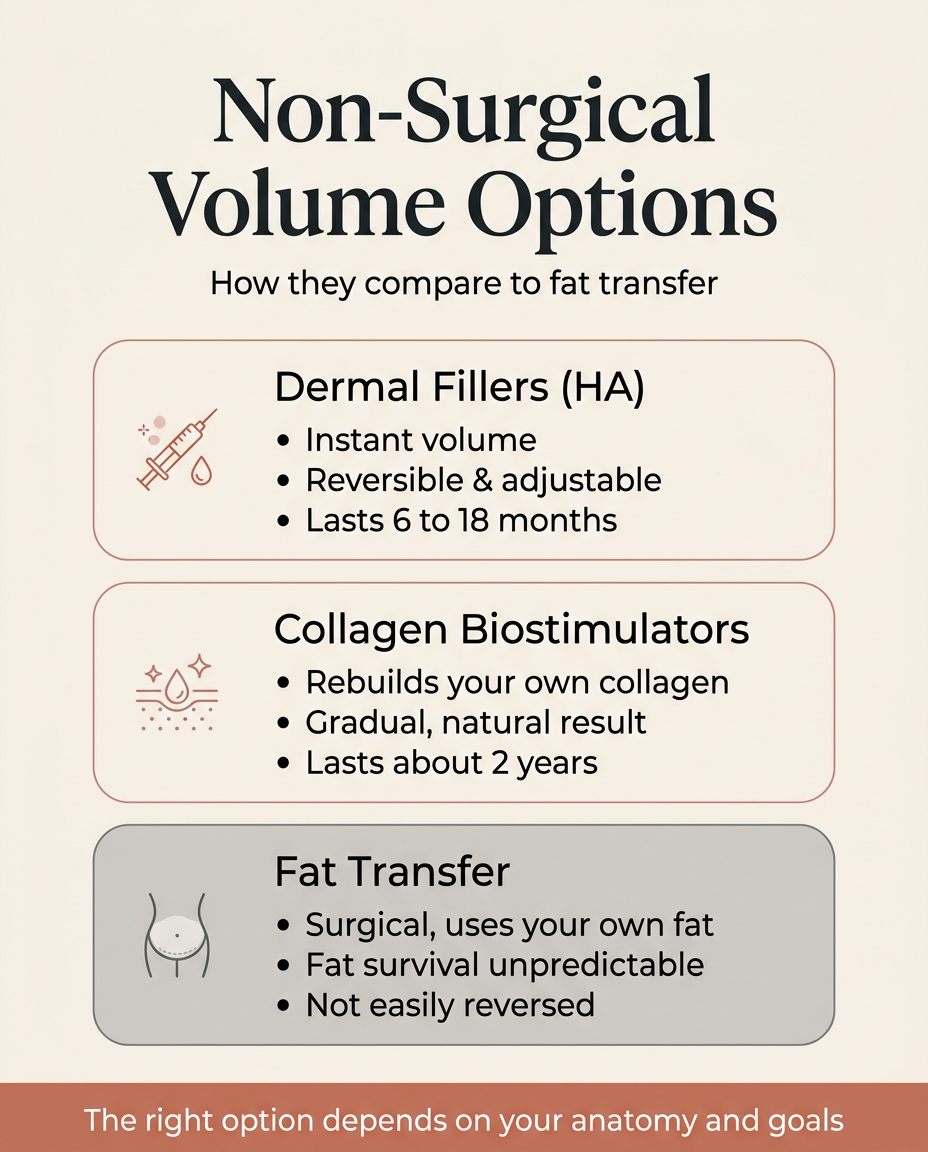
If you have had fat transfer and the result was not what you hoped, or if you are considering fat transfer but want to understand what non-surgical alternatives might achieve, there are several options worth knowing about. None of them are identical to fat transfer — they work through different mechanisms, have different longevity profiles, and suit different clinical situations. But for many patients, they offer a more predictable, more reversible, and easier-to-adjust path to facial volume restoration. The honest answer is that the right choice depends on your anatomy, your goals, and what specifically went wrong (or what you are hoping to avoid).
HA fillers like Restylane and RHA are fully reversible with hyaluronidase — a meaningful advantage when predictability matters. Radiesse (calcium hydroxylapatite) stimulates collagen and provides immediate structural support, particularly well-suited for areas that need lift rather than just volume. Sculptra (poly-L-lactic acid) works differently still — it does not add volume directly but triggers the body’s own collagen production over several months, creating a gradual, natural-looking result that tends to integrate more evenly than injected fat. For patients who had fat transfer and experienced significant resorption, this treatment can often fill the gap that the procedure left — with a much more controlled and predictable outcome. PDO threads offer mechanical lift without adding volume at all, which can be the right answer when the issue is structural laxity rather than volume loss.
| Option | Fat Transfer | HA Filler (Restylane/RHA) | Sculptra | PDO Threads |
|---|---|---|---|---|
| Best for | Patients seeking permanent volume who accept surgical risk | Reversible, precise volume — especially under-eyes and lips | Gradual, diffuse collagen rebuilding — cheeks, temples | Structural lift without volume — jowling, brow, mid-face |
| Mechanism | Living fat cells engraft into tissue | Hyaluronic acid hydrates and lifts dermis | Poly-L-lactic acid stimulates fibroblast collagen | Barbed suture creates mechanical lift + mild collagen response |
| Onset | Weeks–months (post-swelling) | Immediate | 3–6 months gradual | Immediate lift, ongoing collagen 2–3 months |
| Longevity | Permanent (surviving fat) | 6–18 months depending on product | 2–3 years | 12–18 months (lift), collagen longer |
| Reversible | No | Yes (hyaluronidase) | No | No (threads absorb) |
| DB offers | No — referred to plastic surgeon | Yes | Yes | Yes |
Fat Transfer
- Best for
- Patients seeking permanent volume who accept surgical risk
- Mechanism
- Living fat cells engraft into tissue
- Onset
- Weeks–months (post-swelling)
- Longevity
- Permanent (surviving fat)
- Reversible
- No
- DB offers
- No — referred to plastic surgeon
HA Filler (Restylane/RHA)
- Best for
- Reversible, precise volume — especially under-eyes and lips
- Mechanism
- Hyaluronic acid hydrates and lifts dermis
- Onset
- Immediate
- Longevity
- 6–18 months depending on product
- Reversible
- Yes (hyaluronidase)
- DB offers
- Yes
Sculptra
- Best for
- Gradual, diffuse collagen rebuilding — cheeks, temples
- Mechanism
- Poly-L-lactic acid stimulates fibroblast collagen
- Onset
- 3–6 months gradual
- Longevity
- 2–3 years
- Reversible
- No
- DB offers
- Yes
PDO Threads
- Best for
- Structural lift without volume — jowling, brow, mid-face
- Mechanism
- Barbed suture creates mechanical lift + mild collagen response
- Onset
- Immediate lift, ongoing collagen 2–3 months
- Longevity
- 12–18 months (lift), collagen longer
- Reversible
- No (threads absorb)
- DB offers
- Yes
When to Seek a Second Opinion
There’s a hesitation most patients feel after an aesthetic procedure — a reluctance to question the outcome, especially with a surgeon you trusted. I understand that — and I think it’s worth sitting with for a moment before I say what I actually think. Second opinions are one of the most underused tools patients have — and good surgeons are not threatened by them. If you are in any of the following situations, getting an outside evaluation is not a sign of distrust. It is simply good medicine.
- You are more than six months post-procedure and significant asymmetry remains
- You feel firm nodules or lumps that have not diminished over time
- There are skin changes — color, texture, or temperature differences — in treated areas
- You were told to “wait and see” multiple times but the timeline keeps extending
- You have concerns about a potential oil cyst or fat necrosis that have not been formally evaluated
- The result addresses none of your original concerns and you are unsure if revision would help
A consultation at Desert Bloom will not reverse a fat transfer complication — we are not surgeons and we do not pretend to be. But we can help you map what options exist on the non-surgical side, clarify which injectable approaches might complement or address what went wrong, and give you a clearer picture before you make any next decisions. Sometimes the most useful thing a consultation provides is not a treatment plan — it is clarity about what you are actually dealing with.
Frequently Asked Questions
Why doesn't Desert Bloom perform fat transfer?
Can fat transfer complications be reversed?
How long should I wait before deciding the result is final?
Can dermal fillers help if fat transfer didn't give me enough volume?
Is Sculptra better than fat transfer for facial volume?
What questions should I ask a surgeon before a fat transfer procedure?
Can I get fillers or Sculptra while waiting to see my fat transfer results?
If Something Doesn’t Feel Right, You Deserve a Clear Answer
A procedure that did not go the way you hoped is disorienting — especially when it involved surgery, recovery time, and real financial cost. The instinct to minimize (“maybe it’s just not healed yet”), the hesitation to seek a second opinion, the uncertainty about what normal even looks like at this stage — all of it is understandable. What I would gently push back on is the idea that clarity is somehow out of reach. It is not. A good consultation — surgical or otherwise — should leave you understanding exactly what happened, what your realistic options are, and what comes next. That is what you deserve, regardless of where you had your original procedure or what the outcome was.
“Fat transfer is a legitimate procedure — when it goes well, the results can be beautiful and long-lasting. When it doesn't, patients often feel lost because the complications are unfamiliar and the path forward isn't obvious. The most useful thing I can offer in those situations is honest clarity: here's what happened, here's what options exist, here's what I would do. That conversation costs nothing, and it changes everything.”
Related reading: Botched Treatment: When Aesthetic Procedures Go Wrong · Thread Lift Gone Wrong · Dermal Fillers at Desert Bloom · Sculptra Collagen Stimulator · Radiesse · PDO Thread Lift
Individual results vary. This article is for informational purposes only and does not constitute medical advice. Desert Bloom Skincare does not perform fat transfer procedures. Clinical content reviewed by Dr. Natalya Borakowski, NMD. Last updated April 2026.
