Fox Eye PDO Thread Lift | Before & After | Scottsdale, AZ


See real before & after results for fox eye PDO thread lift in Scottsdale. Cat eye lift with threads — cost, recovery, and what to expect at Desert Bloom.
Overview
Let’s talk about what the “fox eye” procedure actually does — because most people arrive having seen it on Instagram, and what they saw there is not what I do here. The sections below cover what PDO threads can realistically achieve at the lateral brow, who makes a good candidate, how the procedure compares to surgical and Botox options, and what recovery actually looks like.
Case Snapshot
- What
- PDO thread lift targeting the lateral brow and outer canthal area to create a subtle upward eye aperture
- Best For
- Mild lateral brow descent, patients seeking a natural outer-eye opening — not a dramatic social-media filter effect
- Lasts
- 12–18 months, with collagen remodeling continuing beyond thread absorption
- At Desert Bloom
- PDO threads placed by Dr. Borakowski; local anesthesia; approximately 30 minutes
- Related Reads
- Non-Surgical Brow Lift · PDO Thread Lift · Thread Lift Gone Wrong · Case Studies
The Instagram Version vs. the Clinical Version

The “fox eye” trend that circulated on social media — the one where models appear to have dramatically pulled, almost alien-like outer corners — is largely a makeup technique, a photograph angle, and in some cases the result of surgical canthopexy performed on faces that were already structurally exceptional. It is not a realistic benchmark for a 30-minute thread procedure. When a patient comes in asking for the “Bella Hadid look,” my first job is to be honest about what that actually means anatomically, and what threads can and cannot do.
What PDO threads can do is genuinely useful: they lift the lateral brow segment, subtly open the outer eye aperture — typically no more than 1 millimeter of elevation — and restore a degree of horizontal tension to the periorbital area that mild descent tends to reduce over time. The result reads as alert and rested — not stretched, not pulled, not filtered. That distinction matters, and I make it at every consultation.
What Happens Anatomically
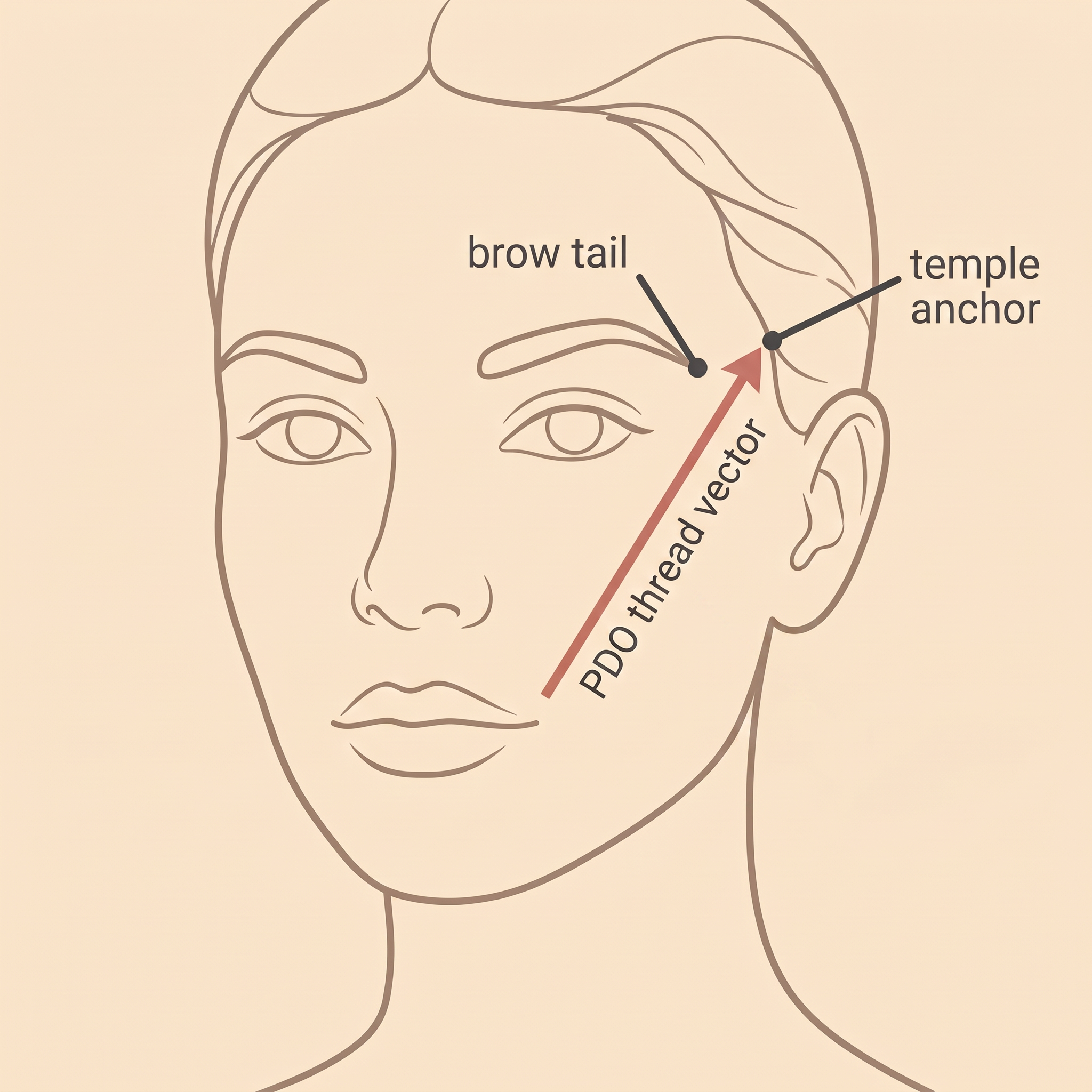
The lateral brow — the tail end of your eyebrow — is anchored by soft tissue that gradually relaxes with age, hormonal shifts, and cumulative sun exposure. As it descends, the outer corner of the eye follows, creating a subtle but noticeable heaviness. PDO threads placed along a specific vector from the temporal hairline toward the lateral brow and outer canthal region physically reposition this tissue. Local anesthesia is applied; the procedure takes roughly 30 minutes. There is no incision, no suture removal later, and no general anesthesia required.
The threads themselves dissolve over several months. What persists longer — and this is the clinically interesting part — is the collagen response they trigger. The body’s repair process around the thread creates a fibrous scaffold that continues to provide subtle support well after the PDO has absorbed. Most patients see the result settle into its final form around the six-week mark, with gradual softening over the following year before a refresh is appropriate.
Who This Is — and Isn’t — Right For
Good candidacy for lateral brow threading is relatively specific. I look for mild to moderate descent — the kind where the outer brow sits lower than it once did, where photographs from five or ten years ago show a noticeably more open outer eye. Skin quality matters too: thread lifting works with tissue that still has some residual elasticity. Patients with significantly lax or heavily sun-damaged skin around the eye may not hold the lift well, and I’ll say that directly in consultation rather than proceed and disappoint.
This procedure is not a replacement for surgical lateral brow lift or canthopexy when those are the anatomically correct solutions. If the degree of descent or the structural anatomy of the brow and eye region genuinely requires surgical correction, I will refer — because the right outcome matters more than a completed appointment. The comparison table below lays out when each approach makes more sense.
Additional contraindications to discuss at consultation include a personal history of poorly controlled diabetes or poor wound healing, and a history of keloid scarring — both of which affect how predictably the skin heals around thread entry points. Fitzpatrick skin types IV through VI are not contraindicated for this procedure, provided there is no elevated keloid risk; Dr. Borakowski reviews skin history and prior reactions individually for each patient.
Comparing Your Options
| Factor | PDO Fox Eye Threads | Surgical Lateral Brow Lift / Canthopexy | Botox Brow Lift |
|---|---|---|---|
| Mechanism | Barbed PDO threads physically reposition lateral brow tissue; collagen remodeling extends the result | Direct tissue repositioning and fixation under general or local anesthesia; permanent structural change | Neurotoxin relaxes depressor muscles, allowing elevator muscles to passively lift the lateral brow |
| Best for | Mild–moderate lateral brow descent; patients wanting a natural, non-surgical lift | Moderate–severe descent; patients ready for permanent correction and surgical recovery | Subtle outer-brow elevation; maintenance between thread sessions; very mild descent |
| Result duration | 12–18 months; refresh at the 12–18 month mark | Long-lasting; years before re-evaluation typically needed | 3–4 months; repeated sessions required |
| Downtime | 2–5 days (swelling, tenderness); most return to normal activity within a week | 1–2 weeks; activity restrictions apply | Minimal; 24–48 hours precautions |
| Dramatic effect possible | No — subtle lift is the realistic ceiling | Yes — structural change allows more significant repositioning | No — limited to a few millimeters of elevation |
| Anesthesia | Local anesthesia only | General or IV sedation typically required | None |
| At Desert Bloom | Yes — Dr. Borakowski | No — surgical referral provided | Yes — combined with threads when clinically appropriate |
PDO Fox Eye Threads
- Mechanism
- Barbed PDO threads physically reposition lateral brow tissue; collagen remodeling extends the result
- Best for
- Mild–moderate lateral brow descent; patients wanting a natural, non-surgical lift
- Result duration
- 12–18 months; refresh at the 12–18 month mark
- Downtime
- 2–5 days (swelling, tenderness); most return to normal activity within a week
- Dramatic effect possible
- No — subtle lift is the realistic ceiling
- Anesthesia
- Local anesthesia only
- At Desert Bloom
- Yes — Dr. Borakowski
Surgical Lateral Brow Lift / Canthopexy
- Mechanism
- Direct tissue repositioning and fixation under general or local anesthesia; permanent structural change
- Best for
- Moderate–severe descent; patients ready for permanent correction and surgical recovery
- Result duration
- Long-lasting; years before re-evaluation typically needed
- Downtime
- 1–2 weeks; activity restrictions apply
- Dramatic effect possible
- Yes — structural change allows more significant repositioning
- Anesthesia
- General or IV sedation typically required
- At Desert Bloom
- No — surgical referral provided
Botox Brow Lift
- Mechanism
- Neurotoxin relaxes depressor muscles, allowing elevator muscles to passively lift the lateral brow
- Best for
- Subtle outer-brow elevation; maintenance between thread sessions; very mild descent
- Result duration
- 3–4 months; repeated sessions required
- Downtime
- Minimal; 24–48 hours precautions
- Dramatic effect possible
- No — limited to a few millimeters of elevation
- Anesthesia
- None
- At Desert Bloom
- Yes — combined with threads when clinically appropriate
Recovery and Results Timeline
Recovery is manageable — but I won’t tell you it’s nothing. Knowing what to expect at each phase prevents the anxiety of interpreting normal healing as a complication.
Days 1–3
Acute Swelling Phase
Localized swelling and tenderness at thread entry points is normal and expected. Avoid strenuous activity, bending forward, and sleeping on the treated side. Cold compresses help — gently, not directly over insertion sites.
Days 4–7
Dimpling Resolves
Minor surface dimpling or skin puckering along thread paths typically softens by end of the first week. This is the thread retracting tissue — it is not a complication. Most patients feel comfortable returning to normal activity by day five.
Weeks 2–4
Soft Tissue Settling
The lateral brow settles into its lifted position as initial inflammatory response resolves. Some patients notice a slightly ‘over-corrected’ appearance in week two that relaxes naturally — this is also normal.
Week 6
Final Result Visible
By six weeks post-procedure the result reflects what the threads have accomplished. This is the right time to assess and photograph. The lift is subtle, natural, and consistent with the patient’s baseline anatomy — not the Instagram filter version.
Months 12–18
The Lift Softens — and That’s Normal
PDO threads have fully absorbed by now. The collagen scaffold they triggered still provides some support, but the lift gradually softens. A refresh session is appropriate in this window for patients satisfied with the initial result.
Frequently Asked Questions
Will I look extreme or 'pulled'?
How is this different from the 'fox eye' trend I've seen online?
When isn't this the right procedure?
Does it hurt?
Can threads be combined with Botox or fillers?
How long do results last, and what happens when the threads dissolve?
Is there anything that affects how well the result holds?
“Thread lifting the lateral brow is one of the procedures where expectation-setting matters as much as technique. The anatomy is unforgiving of over-promise — and patients deserve honesty about what a 30-minute non-surgical procedure can and cannot accomplish.”
This is one of several documented case studies from Desert Bloom Skincare. See all patient case studies →
Individual results vary. Patient consent obtained for case study publication. Clinical content reviewed by Dr. Natalya Borakowski, NMD. Last updated May 2026.
